|
|
| LINKS BACK TO: PALS Personal Pages Index | PALS Front Page | PD Information | Brainteasers | ||||||||||||||||
My Bionic Brain
Where to start?
At the beginning I suppose; where my life with Parkinson��s began and my previous life ended - the moment of recognition. As I watched the Opening Ceremony of the 1996 Olympic Games, little did I realise that my life as I knew it was about to change. I was 44, married, mother of two girls, thinking about re-entering the workforce, but in the meantime occupied by gardening, DIY and interior design. A hands-on kind of gardener/carpenter/painter.
Muhammad Ali walked up to the steps leading to the Olympic Torch and started to climb. I idly watched the arm shake, and suddenly it dawned on me that mine shook in the same way. The commentator said - I can quote the words �� of course he has Parkinson��s��.
The usual consternation, shock, diagnosis, adaptation followed, and I bought every book I could find about it, along with a medical dictionary. Actually, this in no way comes near to the emotional upheaval this brought to our lives, and, not for the first time, I took my husband Liam's reassurance that things would be OK as a sort of mantra, and coped only by shutting out all images of the future, while at the same time reading anything I could lay my hands on about PD!
�� tremor �� slowness of movement (bradykinesia) �� muscle rigidity
and I had lost my automatic arm-swing on the left side, and occasionally tripped while walking.
I was prescribed Sinemet 110, had a bad reaction to it, feeling green with nausea despite slow upward titration of the dose. With the cooperation of my GP, I tried Simenet 125, Sinemet CR, all to no avail. I took Protium (at one time 120mg) , Motilium (up to 30mg a dose), and relied on Gaviscon and Antepsin at various intervals. Sinemet worked extremely well at banishing the symptoms of PD but I could never predict whether I would be just nauseous, or green faced and sweaty with nausea. Nine months later I stopped taking it.
To cut a long story short, my ability to tolerate the medications continued to be poor, though I managed in the end, after an agonising effort to tolerate another dopamine agonist, to take Mirapexin, and Eldepryl, though with the stomach-supporting aids mentioned above.
About two years ago I ran out of time, and the symptoms started to appear over the power of the medications I was taking, and I could only barely tolerate them anyway, so adding anything else in was not an option.
I became increasingly housebound, as my walk had degenerated to the point that, if under enough stress (and stress can temporarily worsen symptoms), my back became totally rigid and painful, my left leg locked, and I could only walk properly backwards, the tremor was sometimes so strong that even sitting on my hand didn��t help �C that just transferred the shaking to the body, foot cramps were frequent and agonising, my facial expression disappeared, my voice became low and monotonous, and my beloved garden was abandoned because I had fallen a few times. I could trim hedges (hand shears), could weed, but couldn��t pick up the cuttings. For DIY I used a little bit of putty on the Phillips screwdriver to hold the screw in place (tremor and carpentry are uneasy bedfellows), but couldn��t screw quickly enough to gain purchase, and so had to try and use my other hand (I am primarily left-handed). Only my stubborn determination kept me going, as each job took longer and longer.
Of course some things suffered: For instance, I had always gone to my daughters' parent-teacher meetings, and it really killed me that, in my younger daughter's last year in school, I had to let Liam go without me.
I had joined a support group for younger people with Parkinson��s �C PALS, which was in turn a branch of the Parkinson��s Association of Ireland. I eventually became their Secretary. I had an interest in web design and created a PALS website. I asked Dr. Timothy Lynch, a Consultant Neurologist in the Mater and Beaumont Hospitals, if he would answer questions emailed in, which he agreed to do.
So there I was, cheering people up over the phone, reading all round me on the internet �C medical journals, anything that would increase my knowledge or understanding of PD, putting together newsletters full of the hope for the future �C research �C plus ways of coping, while all the time I was shutting myself away more and more. I was comfortable in the company of my family or of the other Support Group members. People stare, and can be very rude, and as a relatively young woman, I found this very hard to take. There is a sort of divide you cross when you have a permanent condition - you become a patient psychologically, and healthy people go on the other side. I had always liked being 'pas remarkable', and now that was all gone.
I was beginning to have periods of freezing �C getting suddenly stuck to the ground �C at night or in dark areas.At other times, if I couldn��t walk I could run, but now that was beginning to get out of control because my body would move faster than my legs and I would fall forwards; my left arm was flexed and held in front of me, virtually useless. I would wave like the Queen of England, no cup of tea was safe, and I started to experience blepharospasm or closing of the eyes under stress. I could only go out with someone else. Strangely, once I was sitting down the rigidity in the back disappeared, so for instance I could drive perfectly, but once I got to wherever I was going, I could only walk like a demented peacock.
I had discussed with my neurologist the idea of surgery, as, because of the drug intolerance, I was not getting anything even remotely like adequate control of my symptoms, but he felt the time wasn��t right. I continued on, getting progressively worse �C for the next six months. Friends gradually slipped away, and I threw myself into web design �C the mornings were full of tremor and typos, but by midnight I could type reasonably well. I was lucky in that my right hand was not so badly affected (Parkinson��s typically shows on one side of the body first), That computer saved my sanity. Six months after that first discussion, my neurologist indicated that he thought I would be a suitable candidate for surgery, and said he would write to Mr. Steven Gill at the Frenchay Hospital in Bristol. �C
I was considered a good candidate for surgery because:
If they had not, then surgery would not have been an option, as one has to be levodopa-responsive to benefit from surgery. At no time did I experience dyskinesia, because I was not taking Sinemet or Madopar, but dyskinesia could also be virtually eliminated with surgery.
TOP
In March 2003 I travelled to Bristol, to the Frenchay Hospital, for assessment as to my suitability for surgery. Despite one cancelled flight, and despite the next flight being diverted to Bermingham because of fog, I got there ten minutes before the first assessment, the Neuropsychology Assessment, was due to start!
The second part of the Assessment - the Video Assessment - went well. The ��off-drugs�� and the ��on madopar 250 mg�� segments of the video reduce me to tears still. Off drugs I could hardly move my left hand, and the walking became even more individual than usual, and my face had a mask-like quality Then, when I took the Madopar tablet, I sat waiting for the familiar nausea, which didn��t disappoint. I repeated the series of tests, improving my time for some by as much as 70%, and, once the filming was over, walked and walked between the tests (which were repeated every 20 minutes over three hours). Karen remarked ��I know what it is, she��s enjoying it!�� I cannot think of it now without tears welling up. Just try to imagine what a heady wonderful experience it was, finding my stride, feeling the freedom of the muscles, after what seemed like years of stumbling and lurching. I walked and walked despite the nausea, only giving up when my leg muscles, unused to such normal movement, rebelled.
For a few hours the nausea took second stage to the unbelieveable freedom to move. Liam �C my husband �C who had travelled with me to Frenchay �C arrived, and the delight on his face was something to see. So what did we do �C we �C of course �C went for a walk! By that evening the Madopar had worn off, though not completely, but by the following morning I was back to walking backwards to the bathroom. Tuesday evening came the decision �C it was positive; Mr. Gill would operate, would perform a bilateral Deep Brain Stimulation of the Sub-thalamic nuclei. Text messages were flying back and forth to Ireland, registering our delight and relief and that of our families back home. I don��t know anyone who had so many prayers being said �C in more than one denomination, in various parts of the world.
The operation was long, but under general anaesthetic, and afterwards I was absolutely exhausted. Three days later though, when Karen O��Sullivan, the Parkinson��s Nurse Specialist working with me, switched on the stimulator ( it has to be programmed , which can take some time ), and led me up the middle of the ward, well, what can I say. I walked forwards! Not up straight, but forwards. Despite the incisions, stitches, etc., I knew this was working, though how well only time would tell.
Hopefully the blepharspasm will be temporary. However, in the interim, I arranged to have botox injections on April 3, which take effect in about 10 days from then. I can say now: I walk normally, My typing is getting back to normal (I had gotten used to having a slower left hand; now I am getting used to having a left hand with normal function), I can wave properly, dressing, which used to take longer, especially under time pressure, is back to normal; putting on a jacket doesn��t involve rescuing an arm stuck in the sleeve at an awkward angle; my facial expression is back to normal, my voice has become �C I am told �C more expressive; my DIY skills haven��t improved, but my screwdriver speed is back to normal �C wonder if they have an operation to improve one��s ability to saw in a straight line?
I am still recovering from the surgery and so I nap each day and don��t overdo it �C or try not to.
In my case I had a bilateral implant; in other cases, it may be that unilateral implantation is more appropriate �C on the left side for instance to control symptoms on the right side of the body It��s not cheap �C the technology is cutting edge �C a stimulator, made by Medtronic, rather like a pacemaker, that delivers an electrical pulse via an electrode, to, in my case, the sub-thalamic nucleus, basically knocking out part of its function (it becomes overactive in Parkinson��s, because of the lowered levels of the chemical dopamine), thus restoring a sense of balance. The electrodes are carefully positioned deep within the brain, the wires brought up outside the skull, channelled down the left side of the head behind the ear, underneath the skin, to the stimulator. This is normally inserted behind the collar-bone, but because of my slight build, it was inserted in the abdominal cavity.
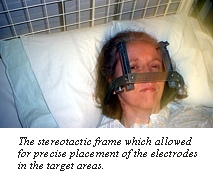
The target is usually about the size of a grain of rice �C one grain of rice on each side of the brain, and the surgeon makes use of MRI scans to check the intended target, while your head is fitted with a frame to hold it steady. Though I am still recovering from the surgery, I can already comment on how my life has been transformed.
I have been lucky enough to have been given my life back. And what is my target now, two weeks after returning home from Bristol? The moon? Carnegie Hall? No, just this: walking to the local newsagent to buy a loaf of bread or a newspaper, and walking home again, by myself. Footnote 1: Four weeks later: Still emotional , but finding myself getting stronger. Had to consult with Frenchay regarding the settings/medication, because, as the brain shrinks back to its normal size after surgery, sometimes this means a slight deterioration in one's performance, but I was told this would happen - it is wise to be prepared as much as possible. Slight adjustments worked and I am back on track. The top of my head is numb, so if I felt the need to scratch an itch, I cannot find the itch in order to scratch it! The extensions need to be kept loose, so moving the neck around gently is advised; otherwise you could limit your head movement. Stress may mean having to take out the patient controller and make a small adjustment to settings; relaxation also. It has been suggested that a weight gain of up to 28 lbs might be expected. Some sites suggest this is because of the elimination of dyskinesia, but in my case I didn't have any. It has been was suggested that weight gain might have an autonomic origin. I seem to have put on about 7 lbs - hopefully that will be all! Footnote 2: I read recently that only 7% of those who could possibly benefit from this surgery have that opportunity��. Footnote 3: Early May: Less tired, but still not able to go a full day, and stress, or talking for a long time, really wears me out. Top of my head still numb, and feels most peculiar - will mention it at my checkup later this month. Well, I was warned that I might put on some weight - about 2 stone in fact, and when I said I had read that this happened becuse of the reduction in dyskinesia, which I didn't have, Karen said she had seen it happen regardless of whether one had dyskinesia or not (mentioned also above)! How right she was - 1.5 stone up so far! 126 lb to 140 lb - Reuters Health News (April 4, 2003) reports on a study done in France which corroborates this... Watch this space June 16 Well, the weight has settled in at about 10 stone (140 lbs), and I have started to watch my food intake - the extra weight isn't killing me but my clothes don't fit! Got up to 147 lb and am now back at 140. Problems with the stimulator settings - at my checkup we went to 180/90/4.2 and 2.0 and I now switch it off at night - counting down to zero first as Karen said I might get a bit of a shock if I switched it on straight to 4.2v. Now setting it at 4.3 and 1.2 - any more than 1.2 for the right side and my eyes and eyebrows start moving independently of me and each other! Have had ups and downs but today it seems to be working fine - not much leeway though in the sense that stress throws it out immediately, my left leg locks and I am back almost (but not quite) where I was before the operation. My meds are now down by 3.6mg Mirapexin - not much, but I seem to be becoming sensitive to it as time post op passes - I hope so, as I would like to have some room to play with before having to try more meds again (disastrous up to now). My typing has improved dramatically and I am thinking about going back to the piano. Three months after the operation I no longer need to nap, but my speech becomes somewhat slurred if I am tired, and sometimes I switch the stimulator off so I can speak! July 28
Weight still the same. New clothes have had to be purchased! Settings now: 90/180/4.2 controlling the left side of the body; 90/180/0.8 to control the right side of the body. Meds: Mirapexin now 0.63mg three times daily. My speech is definitely getting worse - slurring - hard to enunciate clearly at times. To have a decent conversation I just switch the stimulator off. On a positive score though, my walk has gotten more reliable since reducing the meds and since reducing the voltage for the right side of the body - very much so. August 5 The setting of 4.2 volts now 4.9 to work properly (left body side), though I keep to 4.2 around the house. Occasionally, stress leads to gait problems. Mirapexin now 0.88mg (0.7 plus 0.18) three times a day. October 5 After changing the frequency to 220 from 180, we were able to reduce the voltage from 4.9 to 4.5, and I have spent two weeks on holiday in Tuscany, where I was able to walk securely 99 % of the time! Hoping to have some more adjustments made later this month in an effort to sort out the speech. BUT - if I was asked which I would prefer, to have the speech sorted or to be able to be confident of being able to walk, well, there would only be one answer..... October 24 Well, I am still on the same settings after visiting Frenchay, and find that when I have rested and slept well the speech is better than when I am tired....Karen reminded me that I still have PD and may need to get more rest! I gather Medtronic are working on a programmer that can be used over the phone, which will assist those who live far from the hospital where they had DBS in being reprogrammed without having to travel. A version of the main article above was published in Irish Nurse in April 2003, and this is here in the hope that it may assist someone else in finding their way...
AK
| ||||||||||||||||